老年癡呆症是一種不斷進化發展的慢性病,美國國立衛生研究所(NIH)對老年癡呆症的診斷標準進行了進幾十年來的首次修訂。新的診斷標準把老年癡呆症分為三個階段:1)臨床前期;2)輕度認知能力障礙;3)老年癡呆症。
新的診斷標準的應用有利於研究老年癡呆症的病因和病程,對新療法的開發亦有幫助。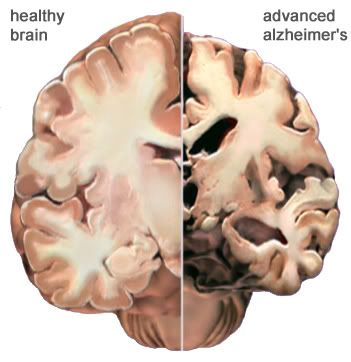
健康人的大腦對比老年癡呆症人的大腦
Alzheimer’s diagnostic guidelines updated for first time in decades
For the first time in 27 years, clinical diagnostic criteria for Alzheimer’s disease dementia have been revised, and research guidelines for earlier stages of the disease have been characterized to reflect a deeper understanding of the disorder. The National Institute on Aging/Alzheimer’s Association Diagnostic Guidelines for Alzheimer’s Disease outline some new approaches for clinicians and provide scientists with more advanced guidelines for moving forward with research on diagnosis and treatments. They mark a major change in how experts think about and study Alzheimer’s disease. Development of the new guidelines was led by the National Institutes of Health and the Alzheimer’s Association.
The original criteria were the first to address the disease and described only later stages, when symptoms of dementia are already evident. The updated guidelines announced today cover the full spectrum of the disease as it gradually changes over many years. They describe the earliest preclinical stages of the disease, mild cognitive impairment, and dementia due to Alzheimer’s pathology. Importantly, the guidelines now address the use of imaging and biomarkers in blood and spinal fluid that may help determine whether changes in the brain and those in body fluids are due to Alzheimer’s disease. Biomarkers are increasingly employed in the research setting to detect onset of the disease and to track progression, but cannot yet be used routinely in clinical diagnosis without further testing and validation.
“Alzheimer’s research has greatly evolved over the past quarter of a century. Bringing the diagnostic guidelines up to speed with those advances is both a necessary and rewarding effort that will benefit patients and accelerate the pace of research,” said National Institute on Aging Director Richard J. Hodes, M.D.
“We believe that the publication of these articles is a major milestone for the field,” said William Thies, Ph.D., chief medical and scientific officer at the Alzheimer’s Association. “Our vision is that this process will result in improved diagnosis and treatment of Alzheimer’s, and will drive research that ultimately will enable us to detect and treat the disease earlier and more effectively. This would allow more people to live full, rich lives without—or with a minimum of—Alzheimer’s symptoms.”
The new guidelines appear online April 19, 2011 in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association. They were developed by expert panels convened last year by the National Institute on Aging (NIA), part of the NIH, and the Alzheimer’s Association. Preliminary recommendations were announced at the Association’s International Conference on Alzheimer’s Disease in July 2010, followed by a comment period.
Guy M. McKhann, M.D., Johns Hopkins University School of Medicine, Baltimore, and David S. Knopman, M.D., Mayo Clinic, Rochester, Minn., co-chaired the panel that revised the 1984 clinical Alzheimer’s dementia criteria. Marilyn Albert, Ph.D., Johns Hopkins University School of Medicine, headed the panel refining the MCI criteria. Reisa A. Sperling, M.D., Brigham and Women’s Hospital, Harvard Medical School, Boston, led the panel tasked with defining the preclinical stage. The journal also includes a paper by Clifford Jack, M.D., Mayo Clinic, Rochester, Minn., as senior author, on the need for and concept behind the new guidelines.
The original 1984 clinical criteria for Alzheimer’s disease, reflecting the limited knowledge of the day, defined Alzheimer’s as having a single stage, dementia, and based diagnosis solely on clinical symptoms. It assumed that people free of dementia symptoms were disease-free. Diagnosis was confirmed only at autopsy, when the hallmarks of the disease, abnormal amounts of amyloid proteins forming plaques and tau proteins forming tangles, were found in the brain.
Since then, research has determined that Alzheimer’s may cause changes in the brain a decade or more before symptoms appear and that symptoms do not always directly relate to abnormal changes in the brain caused by Alzheimer’s. For example, some older people are found to have abnormal levels of amyloid plaques in the brain at autopsy yet never showed signs of dementia during life. It also appears that amyloid deposits begin early in the disease process but that tangle formation and loss of neurons occur later and may accelerate just before clinical symptoms appear.
To reflect what has been learned, the National Institute on Aging/Alzheimer’s Association Diagnostic Guidelines for Alzheimer’s Disease cover three distinct stages of Alzheimer’s disease:
- Preclinical – The preclinical stage, for which the guidelines only apply in a research setting, describes a phase in which brain changes, including amyloid buildup and other early nerve cell changes, may already be in process. At this point, significant clinical symptoms are not yet evident. In some people, amyloid buildup can be detected with positron emission tomography (PET) scans and cerebrospinal fluid (CSF) analysis, but it is unknown what the risk for progression to Alzheimer’s dementia is for these individuals. However, use of these imaging and biomarker tests at this stage are recommended only for research. These biomarkers are still being developed and standardized and are not ready for use by clinicians in general practice.
- Mild Cognitive Impairment (MCI) – The guidelines for the MCI stage are also largely for research, although they clarify existing guidelines for MCI for use in a clinical setting. The MCI stage is marked by symptoms of memory problems, enough to be noticed and measured, but not compromising a person’s independence. People with MCI may or may not progress to Alzheimer’s dementia. Researchers will particularly focus on standardizing biomarkers for amyloid and for other possible signs of injury to the brain. Currently, biomarkers include elevated levels of tau or decreased levels of beta-amyloid in the CSF, reduced glucose uptake in the brain as determined by PET, and atrophy of certain areas of the brain as seen with structural magnetic resonance imaging (MRI). These tests will be used primarily by researchers, but may be applied in specialized clinical settings to supplement standard clinical tests to help determine possible causes of MCI symptoms.
- Alzheimer’s Dementia – These criteria apply to the final stage of the disease, and are most relevant for doctors and patients. They outline ways clinicians should approach evaluating causes and progression of cognitive decline. The guidelines also expand the concept of Alzheimer’s dementia beyond memory loss as its most central characteristic. A decline in other aspects of cognition, such as word-finding, vision/spatial issues, and impaired reasoning or judgment may be the first symptom to be noticed. At this stage, biomarker test results may be used in some cases to increase or decrease the level of certainty about a diagnosis of Alzheimer’s dementia and to distinguish Alzheimer’s dementia from other dementias, even as the validity of such tests is still under study for application and value in everyday clinical practice.
The panels purposefully left the guidelines flexible to allow for changes that could come from emerging technologies and advances in understanding of biomarkers and the disease process itself.
“The guidelines discuss biomarkers currently known, and mention others that may have future applications,” said Creighton H. Phelps, Ph.D., of the NIA Alzheimer’s Disease Centers Program. “With researchers worldwide striving to develop, validate and standardize the application of biomarkers at every stage of Alzheimer’s disease, we devised a framework flexible enough to incorporate new findings.”
http://www.nia.nih.gov/NewsAndEvents/PressReleases/PR20110419guidelines.htm
請閱讀更多我的博客文章>>>