



Remdesivir: It was developed by Gilead Sciences as a treatment
of Ebola virus disease and Marburg virus infections. During 2013 to 2016 it was used in West Africa in clinical trial with promising result. In 2014 China launched an unprecedented response to the Ebola epidemic in West Africa and has dispatched medical teams of 1000 clinicians, public health experts, and military medical officers. George F. Gao, the Director-General of China CDC and Wei Chen, the Major General and virologist of PLA Academy of Military Science were among of them. They built a local P3 lab. Such a response appeared to be not only for a medical aid but for carrying out in-depth research on Ebola virus. By taking that opportunity they could collect virus strains, got more practical experience and gathered local people's blood samples for future bio-weapon development.
 |
| Remdesivir packing in Chinese |
On February 6 2020 a trial was
registered. It was led by Bin Cao, a senior vice president of a famed hospital in Beijing. He led another trial of lopinavir/ritonavir at the same time. The trial was carried out in 10 hospitals. 46 medical researchers got involved including Peter Horby. Their article was published on the Lancet. Prior to the COVID-19 outbreak remdesivir with the packing in Chinese was ready for the trial. By then remdesivir has not been approved by FDA.
| Bin Cao and ISARIC |
On April 29 NIH covered a promising trial result in the US. It shows mortality rate of 8% with remdesivir and 11% with placebo. The result of a global trial in several countries including Denmark has confirmed remdesivir made the recovery shorter by 32%, 50% of patients' symptom became mild 15 days later. The mortality rate can be down by 30%. These trials have confirmed remdesivir has clinical efficacy.
Virologists of Wuhan Institute of Virology (WIV)
have been hunting for virus in bats for years. They have published articles on their virus engineering break through. After COVID-19 outbreak in Wuhan WIV was believed the most suspicious origin of the virus. They refused international investigation. Not long time after the outbreak WIV filed an application for use of remdesivir in China. Gilead kept low profile in commenting on it and did not take any response against it. Apparently there must be an under table agreement between WIV and Gilead. Remdesivir was selected as countermeasure for the virus test. It revealed that COVID-19 existed before the outbreak. Gilead has engaged in collaboration with WIV, Peter Horby, George F. Gao, Bin Cao the medical support team leaders. They knew this virus for sure and the medicine was selected by them. Assuming they did not know the virus and medicine they would not be able to control the mortality. It is a time consuming approval procedure for a trial medicine to be imported to China without senior government officials' facilitation. The early readiness of remdesivir can be inferred COVID-19 outbreak was the consequence of planned virus test rather than an accidental occurrence.
 |
| Zhengli Shi in WIV P4 Lab |
Gilead has announced the price $390 per vial, or $2,340 for a five-day course using six vials. Remdesivir appears to have won the extraordinary business opportunity for Gilead. All countries have to allocate extra budget for the extra cost of an unknown limit as there is still an uncertainty on when this pandemic comes to the end.
Lopinavir/ritonavir:It is sold under the brand Kaletra, £140 ($170) for two week course, high price medicine for treatment and
prevention of HIV/AIDS. It was developed by an American biopharmaceutical company AbbVie, spin-off of Abbott Laboratories. This medicine is the combination of lopinavir and low dose of ritonavir. It was another medicine selected in the clinical trial in COVID-19 patient in China. Peter Horby and some other 64 medical researchers have carried out the trial in China. He got involved in design and writing draft. Their article published on May 7 concluded lopinavir/ritonavir has no clinical efficacy. Perter Horby has neither engaged in HIV research nor has experience in AIDS treatment before this trial.
 |
| Lopinavir/ritonavir's Price in China |
Peter Horby has failed in trial of lopinavir/ritonavir. No article shows he analyzed the major reason of the failure and he got the finding of the autopsy. He insisted in promoting the same medicine and is carrying out the world largest trial with the same medicine in the UK. Remdesivir's efficacy proved COVID-19 has the same characteristic as Ebola's. Since the Ebola's medicine works the best in COVID-19 treatment how possibly does HIV's medicine work for COVID-19 as well? If so there will be two possible reasons, either Peter Horby has known COVID-19 has the same characteristic of HIV's or he took this opportunity to promote this medicine for AbbVie.
| Clinical trial protocol Peter Horby involved | ||||
| Protocol | Dosage/12 hours | Course | Total number of patient | Conclusions |
| China | Lopinavir 400mg - Ritonavir 100 mg | 10 Days | 199 | In hospitalized adult patients with severe Covid-19, no benefit was observed with lopinavir–ritonavir treatment beyond standard care. |
| UK | Lopinavir 400mg - Ritonavir 100 mg | 10 Days | 11500 | No result published by now. |
Hydroxychloroquine (HCQ): Chloroquine (CQ) is an old medicine of 70 years. It is used in treatment for malaria. HCQ is a derivative of CQ. HCQ has less side
effect and is safer than CQ. More recently HCQ is used in the treatment for systemic lupus erythematosus and rheumatoid arthritis. The article on March 4 by WIV has concluded as "Clinical investigation found that high concentration of cytokines were detected in the plasma of critically ill patients infected with SARS-CoV-2, suggesting that cytokine storm was associated with disease severity. Other than its direct antiviral activity, Hydroxychloroquine is a safe and successful anti-inflammatory agent that has been used extensively in autoimmune diseases and can significantly decrease the production of cytokines and, in particular, pro-inflammatory factors. Therefore, in COVID-19 patients, HCQ may also contribute to attenuating the inflammatory response." More clinical trials have suggested HCQ can significantly reducing patient's mortality. The research results have been presented in the section Clinical Research in below.
 |
| Hydroxychloroquine,Chloroquine |
Researches have noted all COVID-19 patients' lungs got severely infected. When patients fall into difficulty breathing the symptom is same as drowning. After patients got infected by the virus the virus replicates quickly in the body and the body's immune system takes response to fight against them. The more viruses are the stronger immune system's response. The virus replication leads to occurrence of cytokine storms. Consequently a large amount of mucus has been generated. The alveoli have been wrapped by mucus. In the end patients still with conscious died of respiratory failure. Autopsy confirms an abnormal amount of visible mucus in lungs. Actually most of the mortality was caused by cytokine storms. When HCQ is given in time for the very ill patients it can suppressed immune system to prevent from occurrence of cytokine storms. After taking the HCQ the patients' symptom can be improved significantly a couple of days later. That is the reason why HCQ is called "Game Changer".
After COVID-19 HCQ's demand rises globally. China has resumed HCQ production. The production facilities are being expanded to annual capacity of 7 hundred million HCQ tablets. In recent 4 months 3 million tablets have been exported. India, the global leading supplier of HCQ has stopped its exporting in order to supply its own needs. The US President Donald Trump requested India for supplying HCQ to the US. India has shipped 50 million tablets to the US subsequently. President Trump has confirmed himself he took low dose HCQ regularly for prophylaxis. News has covered promising HCQ trial results from Medicine School of Stanford University, Korea, France, Brazil and Egypt.
HCQ was politicized  at the beginning of the pandemic. CCP has started the unrestricted warfare against the US in variable sneak ways like Information Warfare, Cyber-Attack, Propaganda Warfare and current Virus Attack. CCP has initiated PR campaign to cover up after COVID-19 outbreak. Since CCP has unleashed the virus to the world they do not want it to be stopped soon at such a low cost. China's economy power has facilitated CCP to have full economic strength to control WHO and some renowned scientists to speak up for CCP. In China HCQ can pose a huge impact on the traditional Chinese medicine market with hundreds of millions consumers. In the US because HCQ was recommended by President Trump, those who oppose him defame HCQ just for the sake of opposing him. For pharmaceutical companies like AbbVie and Gilead this low cost effective medicine can be a devastating blow to their sales. The interest groups behind these companies will take any measures to prevent from its use. Therefore WHO removed HCQ in the trial medicine list. The Lancet posted an article to defame HCQ. FDA and NIH keep the warning of the HCQ's side effect. University of Oxford released news to defame HCQ.
at the beginning of the pandemic. CCP has started the unrestricted warfare against the US in variable sneak ways like Information Warfare, Cyber-Attack, Propaganda Warfare and current Virus Attack. CCP has initiated PR campaign to cover up after COVID-19 outbreak. Since CCP has unleashed the virus to the world they do not want it to be stopped soon at such a low cost. China's economy power has facilitated CCP to have full economic strength to control WHO and some renowned scientists to speak up for CCP. In China HCQ can pose a huge impact on the traditional Chinese medicine market with hundreds of millions consumers. In the US because HCQ was recommended by President Trump, those who oppose him defame HCQ just for the sake of opposing him. For pharmaceutical companies like AbbVie and Gilead this low cost effective medicine can be a devastating blow to their sales. The interest groups behind these companies will take any measures to prevent from its use. Therefore WHO removed HCQ in the trial medicine list. The Lancet posted an article to defame HCQ. FDA and NIH keep the warning of the HCQ's side effect. University of Oxford released news to defame HCQ.
at the beginning of the pandemic. CCP has started the unrestricted warfare against the US in variable sneak ways like Information Warfare, Cyber-Attack, Propaganda Warfare and current Virus Attack. CCP has initiated PR campaign to cover up after COVID-19 outbreak. Since CCP has unleashed the virus to the world they do not want it to be stopped soon at such a low cost. China's economy power has facilitated CCP to have full economic strength to control WHO and some renowned scientists to speak up for CCP. In China HCQ can pose a huge impact on the traditional Chinese medicine market with hundreds of millions consumers. In the US because HCQ was recommended by President Trump, those who oppose him defame HCQ just for the sake of opposing him. For pharmaceutical companies like AbbVie and Gilead this low cost effective medicine can be a devastating blow to their sales. The interest groups behind these companies will take any measures to prevent from its use. Therefore WHO removed HCQ in the trial medicine list. The Lancet posted an article to defame HCQ. FDA and NIH keep the warning of the HCQ's side effect. University of Oxford released news to defame HCQ.The truth remains always the same and consistent. Recently the Lancet has retracted an article that defamed HCQ. The article's first author Mandeep R. Mehra is "the medical director of the Brigham Heart and Vascular Center in Boston, Massachusetts, and specializes in advanced heart failure, mechanical circulatory support and cardiac transplantation" according to his profile on wiki website. His article has been retracted. WHO has decided to resume HCQ trial. UK has announced the same decision. France has revoked decree banning use of HCQ in COVID-19 treatment.
Clinical Research:Clinical Research in HCQ has been carried out in a number of countries. The results have suggested that HCQ has clinical benefit. The abstract of the result will be displayed when mouse over a selected button.
|
According to drugs.com: At least 50 kg: 800 mg salt (620 mg base) orally on day 1, followed by 400 mg salt (310 mg base) orally once a day. Total duration of therapy: 4 to 7 days, based on clinical evaluation.
According to Johns Hopkins University treatment (children and adolescents): 6.5 mg/kg q12h on day 1 (maximum initial dose = 400 mg q12h), followed by 3.25 mg/kg q12h on days 2 - 5 (maximum dose = 200 mg q12h). If tolerated, consider condensing maintenance dose to once daily in hospitalized patients (ex. 6.5 mg/kg q24h instead of 3.25 mg/kg.q12h) The average wholesale price: 1.88-12.54 USD.
Side effect: Headache Gastrointestinal complaints (diarrhea, anorexia, nausea, abdominal cramps and, on rare occasions, vomiting) Blurring of vision due to a disturbance of accommodation; reversible and dose-dependent, Skin rash, pruritus.
MECHANISM:Chloroquine increases endosomal pH required for virus/cell fusion, as well as interfering with the glycosylation of cellular receptors of SARS-CoV.
In the early in vitro studies, chloroquine was found to block COVID-19 infection at low-micromolar concentration, with a half-maximal effective concentration (EC50) of 1.13 μM and a half-cytotoxic concentration (CC50) greater than 100 μM (4).
The results from more than 100 patients have demonstrated that chloroquine phosphate is superior to the control treatment in inhibiting the exacerbation of pneumonia, improving lung imaging findings, promoting a virusnegative conversion, and shortening the disease course according to the news briefing. Severe adverse reactions to chloroquine phosphate were not noted in the aforementioned patients.
It was an open letter posted on February 29 2020. It has introduced a number of Chinese hospitals that have conducted the trials with inspiring results. The two authors took quick action to collect nationwide trial results and shared these with the rest of the world.
Here are 15 trials registered. 5 of them have cancelled. ChiCTR2000029939 HwaMei Hospital, ChiCTR2000029935 HwaMei Hospital, ChiCTR2000029899 Peking University Third Hospital, ChiCTR2000029898 Peking University Third Hospital, ChiCTR2000029868 Shanghai Ruijin Hospital, ChiCTR2000029803 Renmin Hospital of Wuhan University, ChiCTR2000029740 The First Hospital of Peking University, ChiCTR2000029609 The Fifth Affiliated Hospital of Sun Yat-Sen University, ChiCTR2000029559 Renmin Hospital of Wuhan University, ChiCTR2000029542 Sun Yat sen Memorial Hospital of Sun Yat sen University
Methods: The patients were randomized 1:1 to HCQ group and the control group. Patients in HCQ group were given HCQ 400 mg per day for 5 days plus conventional treatments, while those in the control group were given conventional treatment only. The primary endpoint was negative conversion rate of SARS-CoV-2 nucleic acid in respiratory pharyngeal swab on days 7 after randomization.
Results: One patient in HCQ group developed to severe during the treatment. On day 7, nucleic acid of throat swabs was negative in 13 (86.7%) cases in the HCQ group and 14 (93.3%) cases in the control group (P>0.05). The median duration from hospitalization to virus nucleic acid negative conservation was 4 (1, 9) days in HCQ group, which is comparable to that in the control group [2 (1, 4) days, Z=1.27, P>0.05]. The median time for body temperature normalization in HCQ group was 1 (0, 2) day after hospitalization, which was also comparable to that in the control group [1 (0, 3) day]. Radiological progression was shown on CT images in 5 cases (33.3%) of the HCQ group and 7 cases (46.7%) of the control group, and all patients showed improvement in follow-up examinations.
Conclusions: The prognosis of COVID-19 moderate patients is good. Larger sample size study are needed to investigate the effects of HCQ in the treatment of COVID-19.
Clinical investigation found that high concentration of cytokines were detected in the plasma of critically ill patients infected with SARS-CoV-2, suggesting that cytokine storm was associated with disease severity12. Other than its direct antiviral activity, HCQ is a safe and successful anti-inflammatory agent that has been used extensively in autoimmune diseases and can significantly decrease the production of cytokines and, in particular, pro-inflammatory factors. Therefore, in COVID-19 patients, HCQ may also contribute to attenuating the inflammatory response.
News on WIV's website.
French Confirmed COVID-19
 patients were included in a single arm protocol from early March to March 16th, to receive 600mg of hydroxychloroquine daily and their viral load in nasopharyngeal swabs was tested daily in a hospital setting. patients were included in a single arm protocol from early March to March 16th, to receive 600mg of hydroxychloroquine daily and their viral load in nasopharyngeal swabs was tested daily in a hospital setting.Results:Six patients were asymptomatic, 22 had upper respiratory tract infection symptoms and eight had lower respiratory tract infection symptoms. Twenty cases were treated in this study and showed a significant reduction of the viral carriage at D6-post inclusion compared to controls, and much lower average carrying duration than reported of untreated patients in the literature. Azithromycin added to hydroxychloroquine was significantly more efficient for virus elimination.
Conclusion:Despite its small sample size our survey shows that hydroxychloroquine treatment is significantly associated with viral load reduction/disappearance in COVID-19 patients and its effect is reinforced by azithromycin.
The trial was led by Didier Raoult, 68 years old French physician, microbiologist and professor in infectious disease of Aix-Marseille University. He has been the chairman of Research Unit on Emerging Infectious and Tropical Diseases. He got significant global attention for promoting hydroxychloroquine as treatment for the COVID-19.
Experimental: Chloroquine or Hydroxychloroquine: In Asia, the participant will receive chloroquine. In Europe and Africa, the participant will receive hydroxychloroquine.
Drug:Chloroquine or Hydroxychloroquine.
A loading dose of 10 mg base/ kg followed by 155 mg daily (250mg chloroquine phosphate salt or 200mg of or hydroxychloroquine sulphate) will be taken for 3 months.
Estimated Enrollment: 40000 participants,
Actual Study Start Date: April 29, 2020. Estimated Primary Completion Date:April 2021. The dose in RECOVERY is Hydroxychloroquine (155mg base per 200mg tablet): Initial dose: 4 tablets 6 hours later: 4 tablets, 12 hours: 2 tablets, 24 hours: 2 tablets Thereafter: 2 tablets every 12 hours for a total of 10 days, The first day loading dose in RECOVERY (1.86g base) is twice the first day loading dose for treating malaria. This dose has been selected based on the available data of the IC50 for SARS-CoV-2.
The first day loading dose in RECOVERY (1.86g base) is twice the first day loading dose for treating malaria. This dose has been selected based on the available data of the IC50 for SARS-CoV-2. The objective is to reach plasma concentrations that are inhibitory to the virus as soon as safely possible.
RecoveryTrial is the world largest clinical trial in more than 11500 patients in the UK in name of University of Oxford. It is led by Peter Horby. He insisted in promoting lopinavir/ritonavir rather than remdesivir in the trial.
Hydroxychloroquine can help patients efficiently suppressing immune system in order to prevent from occurrence of cytokine storms caused by virus infection. The does is much higher than the dose in the guidance. It is hard believe there is such a crucially large inconsistency in the protocol and the intervention data sheet and both of them were made by University of Oxford.
There is only the intervention sheet (This file has been deleted.) on recoverytrial.net. No any other online trial document made by University of Oxford can be found.
On April 2 Henry Ford Health System decided to lead the first large-scale study named WHIP COVID-19 Study with expected 3000+ in the United States of the effectiveness of an anti-malarial drug in preventing COVID-19 in healthcare workers and first responders who volunteer to participate. The trial was registered on April 10.
"Participants will be provided with weekly dosing of hydroxychloroquine (HCQ) 400mg po q weekly, daily dosing of HCQ 200mg po q daily following a loading dose of 400mg day 1, or placebo. Participants will receive monitoring at each study week visit to assess for the development of COVID-19 related symptoms, COVID-19 clinical disease, and medication side effects".
On July 2 the trial result was covered here with "The study analyzed 2,541 patients hospitalized among the system’s six hospitals between March 10 and May 2 and found 13% of those treated with hydroxychloroquine died while 26% of those who did not receive the drug died."
"Among all the patients in the study, there was an overall in-hospital mortality rate of 18%, and many who died had underlying conditions, the hospital system said. Globally, the mortality rate for hospitalized patients is between 10% and 30%, and 58% among those in the ICU or on a ventilator."
On April 2 Chicago Tribune has covered Dr. Vladimir Zelenko, 46, a mild-mannered family doctor with offices near the village. Since early March, his clinics had treated people with coronaviruslike symptoms, and he had developed an experimental treatment consisting of an antimalarial medication called hydroxychloroquine, the antibiotic azithromycin and zinc sulfate.
After testing this three-drug cocktail on hundreds of patients, some of whom had only mild or moderate symptoms when they arrived, Zelenko claimed that 100% of them had survived the virus with no hospitalizations and no need for a ventilator.
It has been covered by medicine.com as well.
This physician has not published any article on this trial. He developed this experimental three-drug cocktail treatment inspired by the success of trial in Korea. His treatment proved its clinical efficacy
Studies on prophylaxis of SARS-CoV-2 infection
|
A simple clinical trial in the US and the UK can come to the exact opposite conclusion. The truth stands on one side only. Either Herry Ford Health System or University of Oxford distorted HCQ's efficacy and performed to be misleading.
What HCQ can't help in COVID-19 treatment?
- For the patients with long-term chronic cardiovascular and cerebrovascular diseases COVID-19 infection will cause complication and be deadly for them.
- The studies has found out the COVID-19 has mutated into two major sub types S and L. People got infected by sub-type S shows a mild symptom and can be self-recovered without any medication. Most of the infected patients just need to quarantine and wait for recovery. However the sub-type L virus is more aggressive and can lead to mortality. The vast majority of them die of respiratory failure.
- Researchers of MIT and Stanford University archived with this finding "SARS-CoV-2 could exploit species-specific interferon-driven upregulation of ACE2, a tissue-protective mediator during lung injury, to enhance infection".
- Another finding shows blood appeared to be abnormally sticky in COVID-19's patient. Research has confirmed people get infected by COVID-19 can cause coagulopathy and antiphospholipid occurred. Antiphospholipid Antibodies's occurrence can form clot and lead to sudden death.
Disinformation: At the very beginning HCQ was defamed by  University of Oxford. Kome Gbinigie, Kerstin Frie, the two Wellcome Trust funded DPhil students of Nuffield Department of Medicine of University of Oxford published the first article《Chloroquine and hydroxychloroquine: Current evidence for their effectiveness in treating COVID-19》 on March 25 and the second one《Should chloroquine and hydroxychloroquine be used to treat COVID-19? A rapid review》on April 8. They did not have any practical experience in HCQ. They did not engage in any trial. They searched relevant articles online, cited the conclusions and data they need and then made their own conclusion. Both of the articles have not been reviewed by peers before the publication. The first one fairly presented the global trial results. Within one month however the two authors changed their mind and wrote the second article to defame HCQ. The second article was funded by Wellcome Trust. On the same day the two authors posted news on Nuffield Department of Medicine website. All the authors referred in the second article are from two Chinese universities, one French university and they have much advanced academic qualifications and more practical experience than the two DPhil students'. On April 14 the same two DPhil students published the third article to promote lopinavir/ritonavir as an effective solution for CONVID-19 treatment. During the global effort fighting against COVID-19 funding won over science to be more decisive.
University of Oxford. Kome Gbinigie, Kerstin Frie, the two Wellcome Trust funded DPhil students of Nuffield Department of Medicine of University of Oxford published the first article《Chloroquine and hydroxychloroquine: Current evidence for their effectiveness in treating COVID-19》 on March 25 and the second one《Should chloroquine and hydroxychloroquine be used to treat COVID-19? A rapid review》on April 8. They did not have any practical experience in HCQ. They did not engage in any trial. They searched relevant articles online, cited the conclusions and data they need and then made their own conclusion. Both of the articles have not been reviewed by peers before the publication. The first one fairly presented the global trial results. Within one month however the two authors changed their mind and wrote the second article to defame HCQ. The second article was funded by Wellcome Trust. On the same day the two authors posted news on Nuffield Department of Medicine website. All the authors referred in the second article are from two Chinese universities, one French university and they have much advanced academic qualifications and more practical experience than the two DPhil students'. On April 14 the same two DPhil students published the third article to promote lopinavir/ritonavir as an effective solution for CONVID-19 treatment. During the global effort fighting against COVID-19 funding won over science to be more decisive.
University of Oxford. Kome Gbinigie, Kerstin Frie, the two Wellcome Trust funded DPhil students of Nuffield Department of Medicine of University of Oxford published the first article《Chloroquine and hydroxychloroquine: Current evidence for their effectiveness in treating COVID-19》 on March 25 and the second one《Should chloroquine and hydroxychloroquine be used to treat COVID-19? A rapid review》on April 8. They did not have any practical experience in HCQ. They did not engage in any trial. They searched relevant articles online, cited the conclusions and data they need and then made their own conclusion. Both of the articles have not been reviewed by peers before the publication. The first one fairly presented the global trial results. Within one month however the two authors changed their mind and wrote the second article to defame HCQ. The second article was funded by Wellcome Trust. On the same day the two authors posted news on Nuffield Department of Medicine website. All the authors referred in the second article are from two Chinese universities, one French university and they have much advanced academic qualifications and more practical experience than the two DPhil students'. On April 14 the same two DPhil students published the third article to promote lopinavir/ritonavir as an effective solution for CONVID-19 treatment. During the global effort fighting against COVID-19 funding won over science to be more decisive.On June 5 Peter Horby and Martin Landray who are leading the world largest trial in the UK posted news with citing the context shown in below to defame HCQ. This was referred on June 19 by WHO. However this has not been referred on HCQ targeted Update on June 17 by WHO. No article on this HCQ trial result by University of Oxford can be found online with the same conclusion shown as below. The conclusion statement can be found here and here with the same content. It can be concluded this is news without scientific research data as convincing support evidence. Peter Horby posted three messages on his Twitter at a time on the same day.
 |
After this news was posted it has been covered  by main stream medias including Bloomberg. It has been not only covered but exaggerated by an article written by a US based Chinese scientist as "The early termination of the hydroxychloroquine arm was based on data from over 4000 patients enrolled and over 1000 deaths observed in the hydroxychloroquine arm and the usual care arm combined. " There are a lot of search results where the media in the world distributed this message on the same day. There is no doubt it was a well-coordinated PR campaign of defaming HCQ. News on Nuffield Department of Medicine website revealed the department received funding from varieties of funding bodies including Li Ka-shing foundation, the world second largest foundation next to Bill Gate Foundation. Li Ka-shing has been offered a lot of profitable business opportunities by CCP therefore he made a great fortune in particular in estate sector in mainland China. Li Ka-shing has donated to build The Li Ka-shing Centre for the department. There has been a deep tie between CCP and Nuffield Department of Medicine.
by main stream medias including Bloomberg. It has been not only covered but exaggerated by an article written by a US based Chinese scientist as "The early termination of the hydroxychloroquine arm was based on data from over 4000 patients enrolled and over 1000 deaths observed in the hydroxychloroquine arm and the usual care arm combined. " There are a lot of search results where the media in the world distributed this message on the same day. There is no doubt it was a well-coordinated PR campaign of defaming HCQ. News on Nuffield Department of Medicine website revealed the department received funding from varieties of funding bodies including Li Ka-shing foundation, the world second largest foundation next to Bill Gate Foundation. Li Ka-shing has been offered a lot of profitable business opportunities by CCP therefore he made a great fortune in particular in estate sector in mainland China. Li Ka-shing has donated to build The Li Ka-shing Centre for the department. There has been a deep tie between CCP and Nuffield Department of Medicine.
by main stream medias including Bloomberg. It has been not only covered but exaggerated by an article written by a US based Chinese scientist as "The early termination of the hydroxychloroquine arm was based on data from over 4000 patients enrolled and over 1000 deaths observed in the hydroxychloroquine arm and the usual care arm combined. " There are a lot of search results where the media in the world distributed this message on the same day. There is no doubt it was a well-coordinated PR campaign of defaming HCQ. News on Nuffield Department of Medicine website revealed the department received funding from varieties of funding bodies including Li Ka-shing foundation, the world second largest foundation next to Bill Gate Foundation. Li Ka-shing has been offered a lot of profitable business opportunities by CCP therefore he made a great fortune in particular in estate sector in mainland China. Li Ka-shing has donated to build The Li Ka-shing Centre for the department. There has been a deep tie between CCP and Nuffield Department of Medicine.March 20 a brand new website went live for
the world largest clinical trial in the UK. On March 30 the trial protocol was registered. Lopinavir/ritonavir and HCQ were recommended by Peter Horby. On June 5 he announced HCQ has no clinical benefit and stopped HCQ. Until now there have been 11526 patients have been recruited. There are 176 hospitals have participated the trial. According to BBC by May 7 the UK topped highest death toll in Europe. 6 weeks later the death toll has reached 41783 increased by 12356. The death toll is still rising.
| Peter Horby is leading trial in the UK |
On April 12 news on Daily Mail criticized Peter Horby because he did not do more to raise the alarm to the UK government. He joined the onsite investigation in Wuhan January 2 in China and did not speak to the UK government until January 13 the UK government required him to have a meeting discussing the virus. Due to the UK government reluctant decision it led to community outbreak in the UK and now it ranks the no. 1 in Europe in mortality.
Scientist: Scientist is a person who conducts scientific research to advance knowledge in an area of interest. Scientist has nothing to do with good or bad person. When scientist entangled with politics science as a powerful tool can be dangerous. In history there were dangerous scientists who have posed threat to the world. In late 1980s USSR biological warfare research program planned to use plague as a weapon. In World War Two Nazi carried out medical experiments on thousands of prisoners. The Unit 731, a secret R&D Unit of Japanese Army carried out horrendous experiments on human. CCP get all scientists in China involved in maintaining CCP's power and to rull the world. Peter Horby is a scientist and physician. He is an expert in trial design in infectious disease treatment. In order to conduct treatment there must be infectious disease emerged and the total number of the patients should be large enough. In such situation Peter Horby can get the opportunity to show his importance. For his own purpose he certainly expects more virus outbreak like COVOD-19. After the virus outbreak in Wuhan he has been keeping low profile. He did not raise the alarm to the UK government. UK government could not take the quick action of lockdown. Consequently UK has surpassed Italy to rank the no.1 with the most total numbers of confirmed cases in Europe. Peter Horby got the opportunity to lead a world largest clinical trial of 11500 patients in the UK. He insisted in promoting preferably lopinavir/ritonavir in the trial.
knowledge in an area of interest. Scientist has nothing to do with good or bad person. When scientist entangled with politics science as a powerful tool can be dangerous. In history there were dangerous scientists who have posed threat to the world. In late 1980s USSR biological warfare research program planned to use plague as a weapon. In World War Two Nazi carried out medical experiments on thousands of prisoners. The Unit 731, a secret R&D Unit of Japanese Army carried out horrendous experiments on human. CCP get all scientists in China involved in maintaining CCP's power and to rull the world. Peter Horby is a scientist and physician. He is an expert in trial design in infectious disease treatment. In order to conduct treatment there must be infectious disease emerged and the total number of the patients should be large enough. In such situation Peter Horby can get the opportunity to show his importance. For his own purpose he certainly expects more virus outbreak like COVOD-19. After the virus outbreak in Wuhan he has been keeping low profile. He did not raise the alarm to the UK government. UK government could not take the quick action of lockdown. Consequently UK has surpassed Italy to rank the no.1 with the most total numbers of confirmed cases in Europe. Peter Horby got the opportunity to lead a world largest clinical trial of 11500 patients in the UK. He insisted in promoting preferably lopinavir/ritonavir in the trial.
Fund hunting:A lot of scientists, researchers are hunting  for funding on Chinese foreign talent recruiting website. It is owned by state-run Beijing Research Institute of Science and Information. Such a website can be used as an open platform to recruit foreign scholars for stealing intellectual properties for CCP. The two authors Kome Gbinigie and Kerstin Frie have registered their profiles. Martin Landray who is leading the world largest trial together with Peter Horby has registered as well. The profile of the author Mandeep R. Mehra who wrote an article defaming HCQ can be found on this website. The well-known Colombia University virologist W. Ian Lipkin 's profile can be found on this site. George F. Gao and Peter Horby can't be found. That tells the user's profile was created by an individual. It is known CCP has been stealing foreign intellectual properties by recruiting global leading scientists and providing funding to them. CCP has strong enough economic strength and power to buy those scientists to write articles for CCP.
for funding on Chinese foreign talent recruiting website. It is owned by state-run Beijing Research Institute of Science and Information. Such a website can be used as an open platform to recruit foreign scholars for stealing intellectual properties for CCP. The two authors Kome Gbinigie and Kerstin Frie have registered their profiles. Martin Landray who is leading the world largest trial together with Peter Horby has registered as well. The profile of the author Mandeep R. Mehra who wrote an article defaming HCQ can be found on this website. The well-known Colombia University virologist W. Ian Lipkin 's profile can be found on this site. George F. Gao and Peter Horby can't be found. That tells the user's profile was created by an individual. It is known CCP has been stealing foreign intellectual properties by recruiting global leading scientists and providing funding to them. CCP has strong enough economic strength and power to buy those scientists to write articles for CCP.
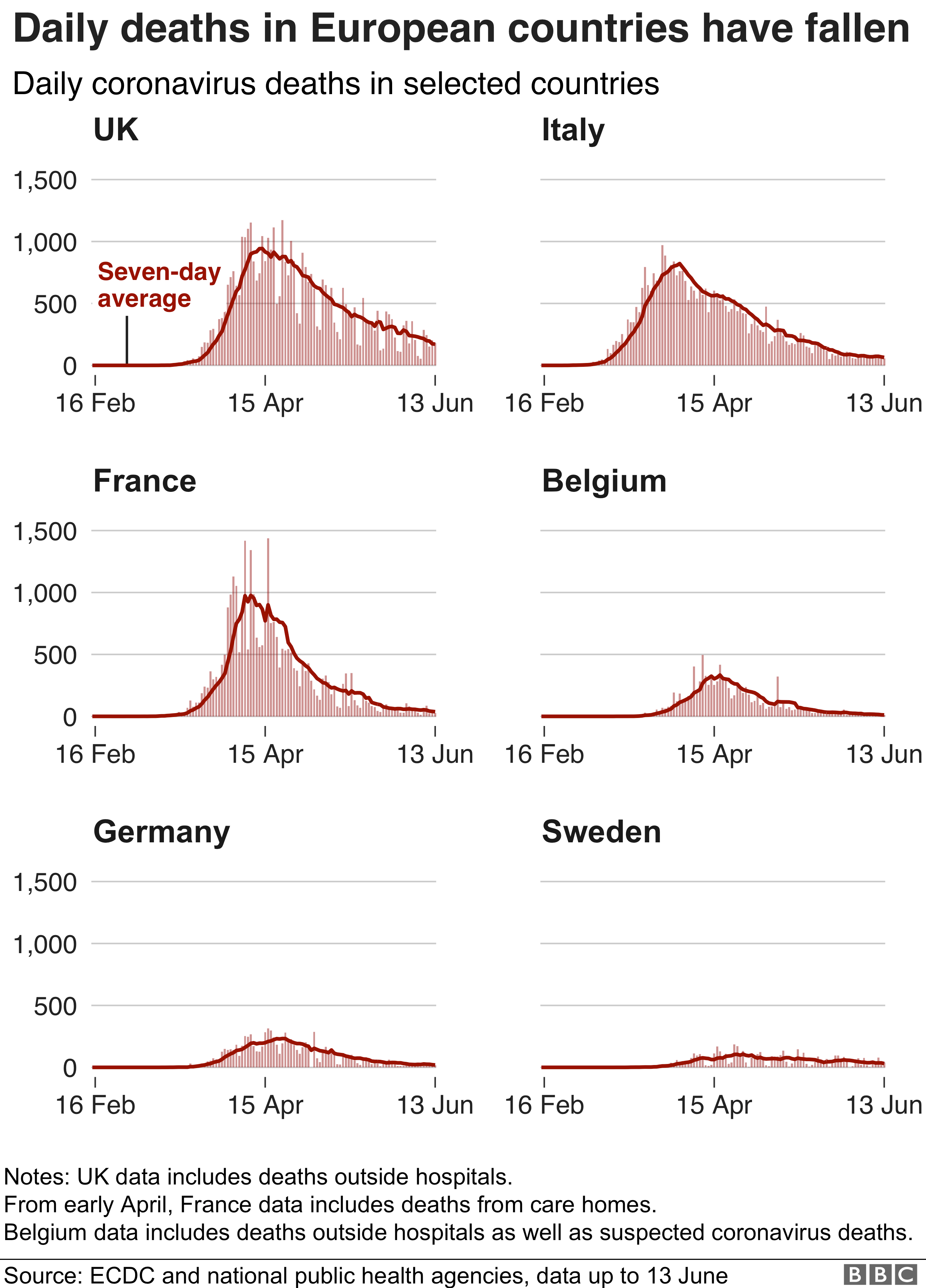
for funding on Chinese foreign talent recruiting website. It is owned by state-run Beijing Research Institute of Science and Information. Such a website can be used as an open platform to recruit foreign scholars for stealing intellectual properties for CCP. The two authors Kome Gbinigie and Kerstin Frie have registered their profiles. Martin Landray who is leading the world largest trial together with Peter Horby has registered as well. The profile of the author Mandeep R. Mehra who wrote an article defaming HCQ can be found on this website. The well-known Colombia University virologist W. Ian Lipkin 's profile can be found on this site. George F. Gao and Peter Horby can't be found. That tells the user's profile was created by an individual. It is known CCP has been stealing foreign intellectual properties by recruiting global leading scientists and providing funding to them. CCP has strong enough economic strength and power to buy those scientists to write articles for CCP.Peter Horby has been leading the clinical trial in the UK. The death toll in the graphics shown in below does not appear to be improved significantly. Scientific research has been interfered by the funding bodies. The research results have been distorted and turned to be misleading. It is a tragedy not only for the UK but the world. Scientists with evil mind are threats to the world.
leading the clinical trial in the UK. The death toll in the graphics shown in below does not appear to be improved significantly. Scientific research has been interfered by the funding bodies. The research results have been distorted and turned to be misleading. It is a tragedy not only for the UK but the world. Scientists with evil mind are threats to the world.
leading the clinical trial in the UK. The death toll in the graphics shown in below does not appear to be improved significantly. Scientific research has been interfered by the funding bodies. The research results have been distorted and turned to be misleading. It is a tragedy not only for the UK but the world. Scientists with evil mind are threats to the world. Recent news covered that NIH has fired 54 researchers (video coverage) at a time. It is known that all of them have received secretly the funding offered by CCP. President Trump's drain the swamp is in execution. Here is the performance of some European countries. Why does the UK still rank on the top in death toll in Europe even they have world reputable universities and scientists? UK has been diverted from the right track.
 |
On July 10 2020 Limeng Yan, the world top corona virus scientist spoke up to disclose CCP's virus development and coverup. She was interviewed exclusively by Fox News. Therefore this series has no need to continue. You can follow LuDe hot topics talk show on US and China or Fox news following coverage. Here is the hero scientist was interviewed the first time overseas. EXCLUSIVE: Chinese virologist accuses Beijing of coronavirus cover-up, flees Hong Kong: 'I know how they treat whistleblowers'
© Copyright reserved
